
Translate this page into:
Access to assistive technology for people with visual impairment

-
Received: ,
Accepted: ,
How to cite this article: Shukla K. Access to assistive technology for people with visual impairment. IHOPE J Ophthalmol 2022;1:79-85.
Abstract
Access to assistive technology (AT) is key to inclusion for people with disabilities in society and its development. Over 2.5 billion people need one or more of these devices globally, but about 1 billion do not have access. Access to these products is even more challenging for people with disabilities. This article reviews national data and government initiatives to understand the present situation of access to assistive technologies and the challenges faced by people with visual impairment in acquiring them. Further, the article discusses the key policy recommendations to enhance access to AT.
Keywords
Assistive technology
Assistive devices
Assistive products
Access
Persons with disabilities
People with visual impairment
People with visual disabilities
Devices for low vision
Accessibility
Disability policy

INTRODUCTION
The 2030 agenda provides a robust framework “to achieve a better and more sustainable future for all people and the world by 2030.” To achieve this, 17 interconnected sustainable development goals (SDGs) have been developed to guide the work for the post-millennium development goal era. One of the main targets is also to address the needs of the most vulnerable and ensure that “no one is left behind.” In the SDGs, issues relevant to disability are referenced in several instances.[1] However, despite the much-needed attention, concerns of people with disabilities continue to be weak,[2] and they face disproportionate levels of poverty; lack of access to education, healthcare, and employment.[2]
The main barriers to inclusion include discrimination and stigma, lack of accessibility in physical and virtual space; lack of access to assistive technology (AT), essential services, and rehabilitation; and lack of support for independent living. This exclusion has not only a social impact but also a tremendous economic consequence. As per a study by the International Labor Organization, the exclusion of people with disabilities from the labor workforce leads to economic loss ranging between 3% and 7% of Gross Domestic Product.[3]
Access to AT by students of any age helps them realize their right to education. When assistive products are used in accessible school settings, students with disabilities are less likely to be marginalized, have more opportunities for social interactions, and achieve a better school environment.[4,5] For instance, access to products such as laptops or tablets with text-to-speech software and magnifiers improves education for students with visual impairments.[6] Access to AT can also reduce inequalities, the need for long-term care, and caregivers’ work.[1]
AT, a subset of health technology, is the application of knowledge and skills related to assistive products, including systems and services. Assistive products include external devices (e.g., smart canes, magnifiers, braille, hearing aids, wheelchairs, mobility devices, and software) especially produced to increase, maintain, or improve the functional capacities, independence, and wellbeing of the individual. Assistive products are often used to prevent impairments and secondary health conditions.[7] People who mostly require AT or assistive devices (AT/AD) are persons with disabilities, the elderly, people with mental health conditions, and gradual functional decline.
According to a recent WHO-UNICEF estimate, over 2.5 billion people need one or more AD. This need will increase to 3.5 billion by 2050, due to the increase in the ageing population, chronic health conditions, and rising non-communicable diseases.[8]
Despite this mounting need, about 1 billion have no access to AT due to high costs, lack of awareness, availability of technology, trained personnel, policy, and financing.[9] Although anyone may require AT/AD, this article focuses on people with disabilities.
INTERNATIONAL AND NATIONAL MANDATES
Globally, the United Nations Convention on Rights of Persons with Disabilities (UNCRPD) mandates the 164 signatories to take effective measures to ensure access to AT for persons with disabilities.[10]
In 2013, at a high-level meeting of the General Assembly on disability and development, the WHO was requested to develop and coordinate a global initiative to realize the obligations under UNCRPD and to increase access to AT. In response to this, in 2014, the WHO established the Global Cooperation on AT, which developed the ‘5P’ People-centered AT model [Figure 1], which provides a bird’s eye view of the AT system. In this model, People’s experiences in the access pathway are determined by four interrelated components: Products, Provision, Personnel, and Policy.

- The 5P people-centered assistive technology model. Source: Policy brief: Access to assistive technology.
Nationally, as obligated, the Rights of Persons with Disabilities (RPwD) Act, 2016 was enacted by the Government of India, which clearly states that appropriate government and local authorities should ensure access to AT as the means for people with disabilities to enjoy equality and non-discrimination. It also calls for specific access to AT/AD for students with disabilities, recreational activities, sports, and infrastructure.[11]
Considering that majority of people who need AT do not have access to it, the Member States of the WHO adopted a resolution in the 71st World Health Assembly to improve access to AT.[12] Among other mandates, Member States requested the Director-General of the WHO to prepare a global report on effective access to AT. Fulfilling this commitment, the WHO and UNICEF jointly prepared and released the Global Report on AT in 2022.[8]
MEASURING ACCESS TO AT FOR PEOPLE WITH VISUAL IMPAIRMENT
To improve access to high-quality and affordable assistive products in all countries, the WHO prepared a priority assistive products list (APL) along the lines of the list of essential medicines. This list contains 50 assistive products selected based on their widespread need and impact on a person’s life; it is a model list for member states to develop a national assistive product list. It can also guide product development, procurement, service delivery, and reimbursement policies.
The International Agency for Prevention of Blindness standard list and essential list[13] of low vision services is also an important and valuable resource that can be adapted to source, compare eye care products, and guide their manufacturing and procurement decisions.
As this paper looks specifically at AT for people with visual impairment, the devices used by persons with visual impairment are extracted from the APL list [Table 1]. [Table 1] also has data from the WHO Rapid AT Assessment survey conducted in December 2021[8] involving 35 countries, including India. A total of 330,000 individuals participated in this survey. Of this, 20.9% of participants reported difficulty in seeing. The prevalence of the need for AT (used by people with visual impairment) is 1.77%; of this, access to products is 14.53%.
| Assistive products | Prevalence of need (in %) | Access to the product (In %) | ||
|---|---|---|---|---|
| Mean | Median (%) | Mode (%) | ||
| Alarm Signalers with light, sound vibration | 0 | 0.08 | 1.76 | 0.61 |
| Audio player with DAISY capability | 0 | 0.03 | 1.67 | 0 |
| Braille display | 0 | 0.01 | 0.76 | 0 |
| Braille writing equipment | 0 | 0.01 | 0.52 | 9.65 |
| Magnifiers (digital/handheld) | 0 | 0.14 | 1.72 | 15.30 |
| Optical magnifiers | 0.01 | 0.32 | 2.84 | 24.20 |
| Recorders | 0 | 0.05 | 1.19 | 0 |
| Screen readers | 0 | 0.02 | 1.20 | 25.00 |
| Mobile phones | 0.02 | 0.18 | 4.41 | 14.70 |
| Spectacles | 4.6 | 18.50 | 65.10 | 53.70 |
| White canes | 0 | 0.09 | 1.38 | 16.70 |
| 0.09 | without spectacle 10.62 | |||
| 1.77 | with spectacle 14.53 | |||
APL: Assistive products list
In all surveyed countries, the need for spectacles was highest among all 50 types of assistive products. The proportion of the population using assistive products was higher in countries with a high Human Development Index (HDI), and access to products increased with HDI.
ASSESSING THE NEED IN INDIA
The situation of AT/AD has been covered by very few studies in India. One of the important ones has been the National Sample Survey (NSS) 2018, and some valuable research has been conducted by those in the fields of education and library sciences which will be discussed further in the article.
The NSS 76th round is the first survey conducted in 2018 after implementing the RPwD Act 2016 – wherein categories of disabilities increased from 7 to 21. As per the survey, the prevalence of disability in India was 2.2%, and the percentage of people with visual disabilities was 0.2%.[14]
NSS is the only national-level survey that captures some information on the means to access AT by persons with disabilities. However, the AT/AD list used in the survey is not comprehensive and does not include crucial ATs required by people with low vision or blindness. The AT/ADs used in the NSS for people with visual disabilities had five items – high-powered glasses, contact lenses, smart canes, regular canes, and others. It may be noted that contact lens is not considered under low vision devices. The list did not include crucial ATs such as magnifiers, braille display and writing equipment, screen readers, alarm signalers, audio players with DAISY capability, mobile phones, and recorders. These are essential APL and are required by people with low vision to function independently.
The method of conducting a survey in the NSS relies on ‘identifying’ disability by an untrained interviewer, which yields low disability estimates, and this is often affected by bias. Moreover, in the case of visual impairments, a clinical assessment is often required. For instance, blindness or functional limitation in vision can be due to cataracts, which can be treated by simple operation and do not need low vision devices. As was seen in a population-level study conducted in Mahbubnagar district in India, in which one of the objectives was to estimate the use, unmet need, and coverage of assistive products based on the self-reported need for three priority APs – distance glasses, hearing aid, and wheelchairs. Of the 60 people who reported needing distance glasses, 25% needed them based on clinical impairment assessment, while 47% needed cataract surgery, and 28% did not have a visual impairment.[15]
In absence of a comprehensive list, it is difficult to generalize findings and adequately assess the unmet need. Even in these five categories of AT used by NSS, the highest acquired AT by people with visual disabilities were high-powered glasses 80.4%; contact lenses 5.9%; smart cane 0.8%; white cane 5%; and other appliances 6.1% [Figure 2]. However, 87.4% of those advised assistive aids had to purchase them, and only 8.2% received any assistance from the government. Around 4.4% acquired assistive aid from NGOs, Charitable organizations, or trusts [Figure 3].
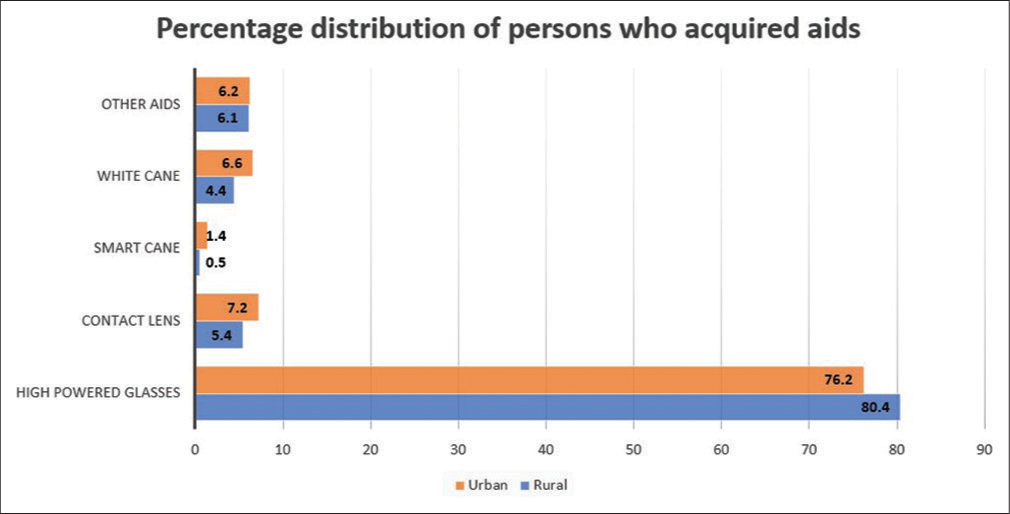
- Types of assistive aids used by people with visual disabilities.
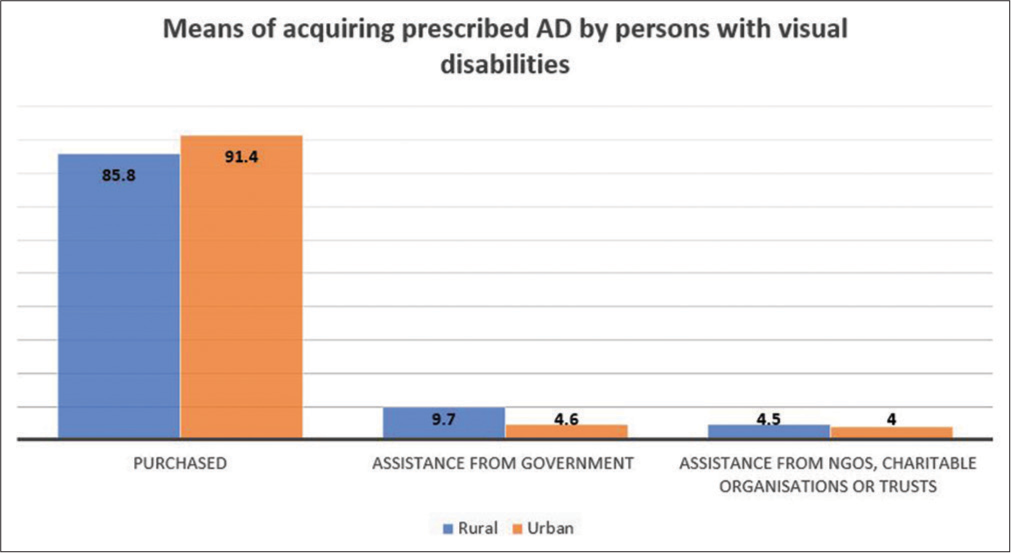
- Means of acquiring prescribed AT/AD.
In a study conducted in blind schools in Delhi, it was seen that the most required ATs by students with visual impairment are talking watches, braille typewriters, audio format, optical and electronic magnifiers, and large computer keyboards.[16] In the same study, it was seen that only 11 out of the 52 ATs were available in 60% or more of the schools. Except for the Braille slate and stylus, the schools had a shortage of AT, highlighting the gap in access.[17]
In another study conducted in schools for blind students in Medinipur and Burdwan districts of West Bengal, it was found that only one institute in each of these divisions uses sufficient resources and ATs. The study also revealed that due to a lack of information and assistance from the Government (both Central and State), the institutions are suffering from a shortage of funds which are leading to hindrance in the overall development of students with visual disabilities. There was also a large variation in the usage of assistive technologies seen in the schools. While braille was the most used, there was considerably lesser availability of other assistive technologies such as sound recorders, talking books, and braille typewriters.[18] In addition to the surveys and statistics, qualitative material and lived experiences also throw light on the importance and need of AD in India for better access to inclusive higher education.[19]
It is difficult to generalize findings based on NSS data, but it does provide critical insights into the gap between demand and supply of AT/AD and the barriers faced by persons with disabilities in accessing them. There are barriers to acquiring prescribed assistive aids, that is, only 31.5% of the persons with visual disabilities (29.8% in rural areas and 37.1% in urban areas) were advised any AT and acquired it, and 14.3 % of the people could not acquire it due to unaffordability, non-availability, and other factors [Figure 4].
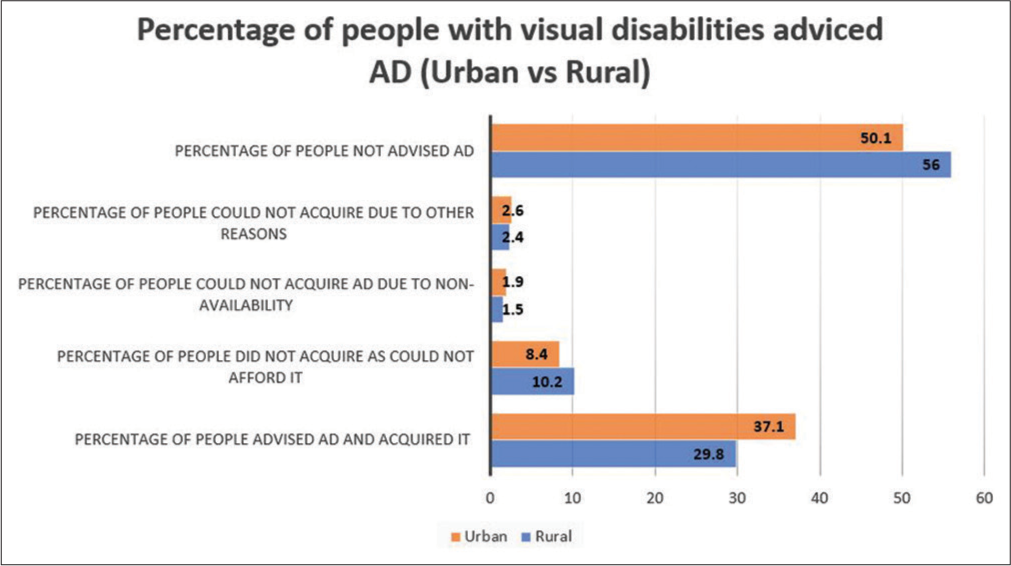
- Percentage of people with visual disabilities advised AT/AD.
This was also seen in studies conducted to understand the barriers to accessing ATs. Non-availability or limited possession of ATs, financial constraints, and lack of awareness are the major barriers to using ATs.[16,17,20]
The Department of Empowerment of Persons with Disabilities (DEPwD), under the Ministry of Social Justice and Empowerment, approves aids/devices for people with disabilities and runs a financial assistance and disbursal scheme called assistance to disabled persons for the purchase/ fitting of aids/appliances (ADIP).
Under the ADIP scheme, eligible people with disability (disability certification percentage of more than 40%) with monthly income from all sources not exceeding 30,000 INR per month are assisted. It means that it is compulsory to have a disability certification percentage of more than 40% and income proof – and people with disabilities face multiple barriers to access these. The NSS data suggest that among the surveyed persons with disabilities, only 28.8% had disability certificates, highlighting the exclusion of people with disabilities in the first step to avail of any government aid and they incur high out-of-pocket expenditure. As can be seen from the data collected, 87.4% of the people purchase the AD from their pocket, and around 13% cannot purchase them due to the high cost of the products.[14]
This financial barrier is inescapable even if a person with a visual disability has certificates and knows which AT will be useful for them. The ADIP scheme provides a device costing up to 15,000 INR for free. For the products in the range of 15,000 INR to 30,000 INR, the government covers only 50% of the cost; for the AT/AD costing more than 30,000 INR, 50% of the cost is covered by the government, which is a case-to-case basis and limited to 20% of the budget under the scheme. Considering the market price of the devices (as per a government document), the devices for low vision cost 110 INR for spectacles; 20,000 INR for screen reading software; 20,000 INR for Daisy player with one speaker; 10,000 INR for handheld electronic magnifiers; 40,000 INR for laptops with screen readers to 1,25,000 INR for refreshable braille display.[21] It may be noted that one person may require more than one appliance/device/ software to be able to function independently, depending on the level of impairment, activities, and needs. Without financial support, people incur considerable out-of-pocket expenditure to access these, which means government aid needs to cover more people.
Yet, the budgetary allocation for this scheme is also reducing over the years. Given that categories of disabilities have increased from seven to 21, the budget also needs to increase proportionally, which is not the case. Moreover, the number of beneficiaries under the scheme has also reduced over the years, [Table 2].[22]
| Year | BE Allocation (in crores) | Revised Estimate | Amount released | No. of beneficiaries |
|---|---|---|---|---|
| 2018–2019 | 220.00 | 223.42 | 216.19 | 30,0865 |
| 2019–2020 | 230.00 | 222.50 | 213.83 | 3,53,629 |
| 2020–2021 | 230.00 | 195.00 | 189.13 | 2,58,749 |
| 2021–2022 (till December 31, 2021) | 220.00 | 180.00 | 121.50 | 1,71,057 |
Another crucial aspect in access to AT is prescription, fitting, user training, and follow-up of AT/AD that requires trained rehabilitation personnel.[23] For instance, training is required to use a white cane, smart cane, braille, screen readers, or other assistive products for a person with low vision. If we exclude spectacles as their usage does not require much training, remaining assistive aids require rehabilitation personnel who can advise appropriate aid and train people in using these products. However, it is seen that due to the shortage of rehabilitation personnel, many people in low-middle-income countries do not have access to assistive products. The density of rehabilitation personnel per 10,000 population is <0.01 in India.[24] Most rehabilitation personnel is concentrated in urban areas or cities, and people in remote areas lack access to rehabilitation services. As can be seen from the data that 56% of the people with visual disabilities in rural areas versus 50.1% in urban areas were not advised of any assistive aid.[14]
As per research conducted in Mysore in higher institutions, it was seen that students with disabilities were familiar with the use of book readers, and magnification equipment, but a large percentage stated the need for training for effectively using JAWS and Braille display. The introduction of a refreshable braille display has helped many students and faculty to read as well as edit text at the same time, but constant training and orientation programs are important to access electronic and print information resources.[25]
It is often said that “what is not counted, does not count,” we need evidence to advocate and plan for intervention and for allocating resources for AT for people with disabilities to uphold the rights of persons with disabilities and maximize their quality of life.
RECOMMENDATIONS TO ENHANCE ACCESS
The DEPwD has done tremendous work on improving access to AT/AD using schemes and enacting the RPwD Act 2016, and soon, the new National Policy on disability will come into place.[26] Nevertheless, ensuring access requires efforts from other ministries as well. Therefore, ministries should synergize their efforts with the DEPwD to ensure resources are not duplicated, and efforts reach maximum people. Following is some of the recommendations to enhance access to AT:
DATA AND SURVEYS
Comprehensive and disaggregated data should be collected as per international standards with a sampling frame covering vulnerable populations to assess the use and unmet need for AT. The data should also capture out-of-pocket expenditure incurred on purchasing, training, and maintenance of AD.
Data are essential to making informed, evidence-based policy decisions, and allocating resources. It will also help in monitoring outcomes of the policy intervention, resources allocated, and decisions for areas requiring improvement, for example, production, pricing, service delivery, procurement, research, and development.
DEVICES AND PRODUCTS
Adopting a list and developing National guidelines and standards specifying products and their description will facilitate in improving product quality, range, price, production, and supply. Using assistive aids, regular follow-ups, maintenance, and repair of devices should be an inherent component of these guidelines.
FINANCING
As most people are purchasing the product from the open market, the government can intervene by improving the economies of scale by bulk purchasing or production to reduce the cost of the devices. Efforts should be directed to create awareness about schemes that provide free and subsidized products.
STRENGTHEN REHABILITATION SERVICES
The Ministry of Health and Family Welfare and the Ministry of Social Justice and Empowerment should work collaboratively to integrate rehabilitation into all levels of healthcare. Furthermore, ministries should work together to expand the seats for training and capacity building of the rehabilitation professionals.
The disaggregated data on spending on rehabilitation services by the people should be collected so that adequate funds to cover these services under the national insurance scheme can be made. Wherever internet facilities are available, telerehabilitation services should be strengthened to allow more people to receive rehabilitation services and get prescriptions for devices remotely.
INVOLVE PEOPLE WITH DISABILITIES IN PLANNING
Active involvement of persons with disabilities and their caregivers helps bring useful experience about challenges that they face and insights about possible solutions. Hence, active consultation should be organized to understand the need while planning AT services. They can also be ambassadors of change and peer supporters who can help others who need access to devices.
Declaration of patient consent
Patient’s consent not required as there are no patients in this study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Assistive products and the sustainable development goals (SDGs) Global Health. 2016;12:79.
- [CrossRef] [PubMed] [Google Scholar]
- The Price of Exclusion: The Economic Consequence of Excluding People with Disabilities from the World of Work In: Employment Working Paper, Skills and Employability Department. 2009. p. :3-97.
- [Google Scholar]
- The Impact of Asssitive Technology on the Educational Performance of Students with Hearing Impairment: A Rapid Review of the Research In: Global Perspectives on Assistive Technology: Proceeding of the GReAT Consultation. Geneva: World Health Organization; 2019. p. :22-3.
- [Google Scholar]
- Connecting to Learn: Educational and Assistive Technology for People with Disabilities. Washington, DC: American Pyschological Association; 2004.
- [CrossRef] [Google Scholar]
- WIPO Technology Trends. 2021. Geneva: World Intellectual Property Organization; Available from: https://www.wipo.int/edocs/pubdocs/en/wipo_pub_1055_2021.pdf [Last accessed on 2022 Jun 30]
- [Google Scholar]
- Improving Access to Assistive Technology for Everyone, Everywhere France: World Health Organization; 2016.
- [Google Scholar]
- Global Report on Assistive Technology Geneva: World Health Organization and United Nations Children’s Fund; 2022.
- [Google Scholar]
- Fact Sheets/Assistive Technology. Available from: https://www.who.int/news-room/fact-sheets/detail/assistive-technology [Last accessed on 2018 May 18]
- [Google Scholar]
- United Nations Department of Economic and Social Affairs. United Nations. Available from: https://www.un.org/development/desa/disabilities/convention-on-the-rights-of-persons-with-disabilities.html [Last accessed on 2022 May 06]
- [Google Scholar]
- Department of Empowerment of Persons with Disabilities. In: The Rights of Persons with Disabilities Act. New Delhi: DEPwD, Ministry of Social Justice and Empowerment; 2016.
- [Google Scholar]
- 71.8. Improving Access to Assistive Technology Geneva: World Health Assembly; 2018.
- [Google Scholar]
- International Agency for the Prevention of Blindness. 2017. Available from: https://www.valuedsupplier.iapb.org/media/uploads/2021/03/iapb-essential-list-for-low-vision-services-v1-march-2017.pdf [Last accessed on 2022 Aug 09]
- [Google Scholar]
- Persons with Disabilities in India: NSS 76th Round New Delhi: Ministry of Statistics and Programme Implementation, Government of India; 2018.
- [Google Scholar]
- Estimating assistive product need in Cameroon and India: Results of population-based surveys and comparison of self-report and clinical impairment assessment approaches. Trop Med Int Health. 2021;26:146-58.
- [CrossRef] [PubMed] [Google Scholar]
- Barriers to using assistive technology among students with visual disabilities in schools for the blind in Delhi, India. Disabil Rehabil Assist Technol. 2021;16:802-6.
- [CrossRef] [PubMed] [Google Scholar]
- Assistive technology for students with visual disability in schools for the blind in Delhi. Disabil Rehabil Assist Technol. 2020;15:663-9.
- [CrossRef] [PubMed] [Google Scholar]
- Use of Assistive Technology in Blind Schools of West Bengal: A Comparative Study In: Library Philosophy and Practice, Paper. 2018.
- [Google Scholar]
- Department of Empowerment of Persons with Disabilities. New Delhi: Ministry of Social Justice and Empowerment; Available from: https://www.bit.ly/3R8ySO0 [Last accessed on 2014 Jul 23]
- [Google Scholar]
- DEPWD Annual Report (2021-2022) New Delhi: Department of Empowerment of Persons with Disabilities, Ministry of Social Justice and Empowerment; 2021.
- [Google Scholar]
- Health Topics/Assistive Technology. Geneva: World Health Organization; Available from: https://www.who.int/health-topics/assistive-technology#tab=tab_1 [Last accessed on 2022 Jul 05]
- [Google Scholar]
- Health-related rehabilitation services: Assessing the global supply of and need for human resources. BMC Health Serv Res. 2011;11:276.
- [CrossRef] [PubMed] [Google Scholar]
- Information technology for the visually challenged library users. J Libr Inform Commun Technol. 2014;6:1-14.
- [Google Scholar]
- Disabilities. 2022. Available from: https://www.disabilityaffairs.gov.in/upload/uploadfiles/files/draft%20copy%20new%20national%20policy%20may%202022%20.pdf [Last accessed on 2022 Jun 26]
- [Google Scholar]




